by Carlton Brown | Dec 1, 2022 |
Download a copy of the: (1) Evidentiary Document referred to in this Open Letter (PDF: EvidentiaryDocument_COVID19NationalLevelHarm_01122022, MS Word (clickable citations): EvidentiaryDocument_COVID19NationalLevelHarm_01122022), (2) Slide Deck of Evidentiary Document including annotated graphics EvidentiaryDocument_COVID19NationalLevelHarm_Slidedeck_01012023, and (3) associated study results and graphics (ADE_VAED_Vaccine-failure), (Toxic COVID-19 vaccine Lots (VEARS, USA))
Open Letter & Evidentiary Document for the Prime Minister and all Ministers: COVID-19 negative vaccine effectiveness and harm evidence in New Zealand and overseas (Results, Call to Action)
To: “j.ardern@ministers.govt.nz” <j.ardern@ministers.govt.nz>, “a.little@ministers.govt.nz” <a.little@ministers.govt.nz>, “p.henare@ministers.govt.nz” <p.henare@ministers.govt.nz>, “a.verrall@ministers.govt.nz” <a.verrall@ministers.govt.nz>, “a.sio@ministers.govt.nz” <a.sio@ministers.govt.nz>
Cc: “c.sepuloni@ministers.govt.nz” <c.sepuloni@ministers.govt.nz>, “c.hipkins@ministers.govt.nz” <c.hipkins@ministers.govt.nz>, “d.oconnor@ministers.govt.nz” <d.oconnor@ministers.govt.nz>, “d.parker@ministers.govt.nz” <d.parker@ministers.govt.nz>, “d.clark@ministers.govt.nz” <d.clark@ministers.govt.nz>, “m.woods@ministers.govt.nz” <m.woods@ministers.govt.nz>, “g.robertson@ministers.govt.nz” <g.robertson@ministers.govt.nz>, “j.shaw@ministers.govt.nz” <j.shaw@ministers.govt.nz>, “j.tinetti@ministers.govt.nz” <j.tinetti@ministers.govt.nz>, “k.davis@ministers.govt.nz” <k.davis@ministers.govt.nz>, “k.mcanulty@ministers.govt.nz” <k.mcanulty@ministers.govt.nz>, “k.allan@ministers.govt.nz” <k.allan@ministers.govt.nz>, “m.davidson@ministers.govt.nz” <m.davidson@ministers.govt.nz>, “m.whaitiri@ministers.govt.nz” <m.whaitiri@ministers.govt.nz>, “m.wood@ministers.govt.nz” <m.wood@ministers.govt.nz>, “n.mahuta@ministers.govt.nz” <n.mahuta@ministers.govt.nz>, “p.twyford@ministers.govt.nz” <p.twyford@ministers.govt.nz>, “p.williams@ministers.govt.nz” <p.williams@ministers.govt.nz>, “p.radhakrishnan@ministers.govt.nz” <p.radhakrishnan@ministers.govt.nz>, “s.nash@ministers.govt.nz” <s.nash@ministers.govt.nz>, “w.jackson@ministers.govt.nz” <w.jackson@ministers.govt.nz>, “cabinetoffice@dpmc.govt.nz” <cabinetoffice@dpmc.govt.nz>, “covid19vaccinesafetynz@protonmail.com” <covid19vaccinesafetynz@protonmail.com>
Dear Rt Hon Jacinda Ardern, Prime Minister, Hon Andrew Little, Minister of Health, Hon Dr. Ayesha Verrall, Minister of COVID-19 Response, and Hon Peeni Henare and Hon Aupito William Sio, Associate Ministers of Health
In this Open Letter and evidentiary document, I share my research results on overseas government and Ministry of Health (MoH) COVID-19 vaccine surveillance and pharmacovigilance data indicating irreparable vaccine-induced harm. Furthermore, I share important evidence that SARS-CoV-2 originated from gain-of-function research, remind you that no evidence exists for an animal-to-human origin, and highlight that its potential source lay beyond Wuhan, China. A series of requests for investigations are made below linked to this evidence, including the statistical biases evident in the Ministry of Health and other healthcare agencies’ calculable unvaccinated COVID-19 case rates. These biases essentially eliminated the negative vaccine effectiveness harm signal from ready public view. This evidentiary document is provided by a former European corporate venture capital-funded CEO/vaccine innovator (“Vaccines for Mutating Viruses”), veterinarian with 36 years of vaccine use experience, and a private researcher. It is supported by 525 unique data, scientific, and other citations.
According to New Zealand, England, Scotland, and Canada healthcare agencies and Global surveillance data (77 nations), these vaccines failed to prevent SARS-CoV-2 infection as initially touted. Significant negative vaccine effectiveness and vaccine failure were evident with the emergence of antigenically distinct strains (i.e., Delta, Omicron). The vaccine industry experienced antibody-dependent enhancement of virus infection (ADE) and vaccine-associated enhanced disease (VAED) with three other different coronaviruses and their spike protein vaccine prototypes in the last 30 years, giving my study results a predictable context. Furthermore, one year of US lot-numbered COVID-19 vaccine-associated deaths and hospitalizations equaled 32x (Comirnaty 15.4x) and 20x (Comirnaty 10.5x) of all US vaccine-associated deaths and hospitalizations, respectively. These adverse outcomes were highly skewed and peaked across vaccine lots and were associated with a minority of lots sent to a larger number of US States. This data highlights that there was an urgent need for investigation by the US and other regulatory and healthcare agencies before expanded population use.
A vast chasm exists between the vaccine safety and efficacy experienced in 2021-2022 and the falsifiable 95% vaccine efficacy and safety proclaimed by governments with Comirnaty’s first Emergency Use Authorization in 2020 (USA). This document reviews critical pharmacotoxicology and clinical safety package deficiencies evident in overseas regulatory reviews. This helps explain why Pfizer then struggled to cope with the sheer volume of Comirnaty adverse event reports in the first 90 days post-launch. This was uncharacteristic of a safe vaccine. Numerous vaccine-associated enhanced disease mechanisms are evident by which vaccine spike proteins can cause disease or exacerbate comorbidities common to severe COVID-19 outcomes. These mechanisms place upregulated furin and angiotensin-converting enzyme-2 receptors (ACE2) and prevalent comorbidities in tissues and organs common to all three center-stage. At the same time, SARS-CoV-2’s spike protein provides its uniquely encoded furin cleavage site for the furin to cleave its S1 and S2 sub-units and activate its ACE2-receptor-mediated infectivity and pathogenicity.
Of grave concern for global public health is a gain-of-function origin to SARS-CoV-2 is indicated by its spike protein incorporating human infectivity and pathogenicity enhancing features unprecedented in nature while synthetic biology left its fingerprints. Furthermore, there is no evidence supporting a Wuhan Huanan market zoonosis because no virus progenitor or animal host was ever identified. There are two reasons for detailing a coronavirus gain-of-function origin to SARS-CoV-2. Firstly, the negative vaccine effectiveness evident in governments’ COVID-19 surveillance data could have been enhanced by a genetically modified SARS-CoV-2. Secondly, the world will be left vulnerable to future pandemics if there was no accidental release from the Wuhan Institute of Virology. At least two other potential SARS-CoV-2 origins exist beyond Wuhan, with one of these potentially involving a WHO, Five Eyes, and NATO-spearhead member nation connected with Ukraine.
The US Department of Defense (DoD) and National Institutes of Health (NIH) funding of EcoHealth Alliance (EHA, $69 million) and its connections one-degree-removed were scrutinized because EHA’s leader led a failed attempt to cover up SARS-CoV-2’s gain-of-function origin. EHA directed research that genetically modified bat SARSr-CoVs that could not infect humans so that they could. EHA’s $14.2 million funding application to the DoD in 2018 showed its intent to insert a codon-optimized furin cleavage site (FCS) into bat SARSr-CoVs. A uniquely encoded Arginine-doublet containing FCS now sits between SARS-CoV-2’s spike protein S1 and S2 sub-units, which has no precedent in known viruses and may have infringed patents. Besides EHA’s long-standing collaborations with two coronavirus gain-of-function research epicenters in the USA and China, it had another with Metabiota. Metabiota’s Series-A lead investor was a Hunter Biden part-owned investment firm. The DoD-funded Metabiota operated in Pentagon Biolabs in Ukraine and US-funded Biolabs in Cameroon and researched corona-, monkeypox-, influenza-, and Ebola viruses. Metabiota has implemented major DoD and Homeland Security contracts across Central Africa while its surveillance role in Sierra Leone’s Ebola outbreak in 2014 created significant controversies.
You are requested to investigate: (1) this New Zealand and overseas evidence for negative vaccine effectiveness, vaccine failure, and toxic vaccine lots, (2) the statistical biases evident in the MoH and other healthcare agencies’ calculable unvaccinated COVID-19 case rates, which essentially eliminated the negative vaccine effectiveness signal, (3) the role of COVID-19 vaccination in exacerbating comorbidities most frequently associated with serious-severe COVID-19 outcomes, (4) SARS-CoV-2’s gain-of-function origin while internationally championing a punitive global ban on gain-of-function R&D, and (5) the conduct of the WHO during COVID-19 linked to seven critical points detailed in section 2.7. Would you please ensure New Zealanders are updated on their recently acquired life-long health risks and that informed consent guidelines associated with COVID-19 vaccination be urgently amended? Would government please prioritize clinical research into COVID-19 antibody-dependent enhancement of virus infection, vaccine-associated enhanced disease, and antigenic imprinting in the New Zealand population? Thank you.
Yours sincerely
Dr. Carlton Brown BVSc (1986, Massey University), MBA (1997, London Business School).
Former CEO and co-innovator at Immune Targeting Systems Ltd (UK), “Vaccines for Mutating Viruses.”
Raising awareness for antibody-dependent enhancement of virus infection (ADE), vaccine-associated enhanced disease (VAED), and antigenic imprinting.
https://www.linkedin.com/in/carlton-brown-13b66232/, https://orcid.org/0000-0003-4871-7521, https://substack.com/profile/113761363-carlton-b-brown, https://twitter.com/ADE_Bioweapon.
Download the Evidentiary Document: https://grandsolarminimum.com/2022/12/01/covid-19-vaccine-harm-evidence/.
by Carlton Brown | Dec 13, 2020 |
It is vitally important the public is made aware of the potential downstream health risks associated with SARS-CoV-2 vaccination. Normality has been bypassed to expedite a SARS-CoV-2 vaccine for emergency use authorization (EUA) with the MHRA, EMA, FDA, and other national drug regulatory agencies around the world.
There is a sound scientific basis to petition governments to prevent them enforcing SARS-CoV-2 immunization on the general population, until the full safety and efficacy is understood. Citizens should have a choice. The use of reverse transcription polymerase chain reaction (RT-PCR) at amplification cycle thresholds (Ct) exceeding 35, without genome sequencing to confirm false positives, means any disease morbidity-mortality data so derived is questionable both for vaccine studies and more generally (see below).
Remember, seasonal flu attacks 10-20% of the population each year and kills a similar percentage to SARS-CoV-2, while Influenza pandemics infect >30% of the world’s population (with varying mortality rates from <1% to 2.5% for the 1918 Spanish flu). This week (10/12/2020) 0.88% of the world had been diagnosed as infected with SARS-CoV-2. For clarity, this pandemic is real (technically). However, one must dis-aggregate bonafide disease and mortality data from the high false-positive data acquired using RT-PCR with the Ct >35-40 in asymptomatic and co-morbid disease sub-populations, or false SARS-CoV-2 diagnostic labels put on other causes of mortality.
Key vaccine safety and efficacy information (so far):
- SAFETY: (1) The FDA published a list of 21 potential adverse events https://www.fda.gov/media/143557/download (2) General guidance to Industry: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/development-and-licensure-vaccines-prevent-covid-19
- CLINICAL DATA: (1) Pfizer-BioNTech COVID-19 Vaccine data (BNT162b2): Vaccines and Related Biological Products Advisory Committee Meeting December 10, 2020. FDA Briefing Document https://www.fda.gov/media/144245/download.
- “Most COVID-19 candidate vaccines express the spike protein or parts of the spike protein, i.e., the receptor binding domain (RBD), as the immunogenic determinant.”
- Vaccine efficacy definition (VE): (1) Primary efficacy endpoint for BNT162b2 against confirmed COVID-19 was evaluated in participants without evidence of prior SARS-CoV-2 infection prior to 7 days after Dose 2. (2) Assessments for illness visits included a nasal (mid-turbinate) swab, which was tested at a central laboratory using a RT-PCR test (i.e., Cepheid; FDA authorized under EUA, or other sufficiently validated nucleic acid amplification-based test (NAAT) to detect SARS-CoV-2, PLUS at least one of the following symptoms: fever; new or increased cough; new or increased shortness of breath; Chills; new or increased muscle pain; new loss of taste or smell; sore throat; diarrhea; vomiting (i.e., non-specific flu-like and gastrointestinal symptoms).
- COMMENT: Dr. Michael Yeadon, former Chief Scientific Officer and VP for Pfizer Allergy Respiratory Research and others petitioned the European Medicine Agency (EMA, Netherlands, EMA Petition PDF). This petition detailed major issues with the use of RT-PCR defined in the study protocol to diagnose cases of SARS-CoV-2: QUOTE: “These test kits referred to in the trial protocol, namely the Cepheid Xpert Xpress SARS-CoV-2, the Roche Cobas SARS-CoV-2 real-time RT-PCR test (EUA200009/A001), and the Abbott Molecular/Real-Time SARS-CoV-2 assay (EUA200023/A001), are very unreliable tools when they are used to determine whether the nasal swab sample collected from a symptomatic participant contains SARS-CoV-2 or not. These real-time RT-PCR or RT-quantitative PCR tests should be referred to as rRT-PCR or RT-qPCR tests to be distinguished from conventional RT-PCR. The very short RT-qPCR product (amplicon) cannot be analyzed by automated Sanger sequencing as the products of conventional PCR can. And DNA sequencing for validation of the PCR products is needed to correctly determine if the presumptive RT-qPCR-positive SARS-CoV-2 test result is a true positive or a false positive.”
- EFFICACY: In the planned interim and final analyses, vaccine efficacy 7 days after Dose 2 was 95%, (95% CI 90.3; 97.6) in participants without prior evidence of SARS-CoV-2 infection and >94% in the group of participants with or without prior infection. Efficacy outcomes were consistently robust (≥93%) across demographic subgroups (VE was 74.4% in Asian subjects).
- SAFETY: (1) A higher proportion of vaccine recipients reported adverse events compared with placebo recipients, and this imbalance was driven by reactogenicity after vaccine injection. (2) The most common solicited adverse reactions were injection site reactions (84.1%), fatigue (62.9%), headache (55.1%), muscle pain (38.3%), chills (31.9%), joint pain (23.6%), fever (14.2%); severe adverse reactions occurred in 0.0% to 4.6% of participants, were more frequent after Dose 2 than after Dose 1, and were generally less frequent in participants ≥55 years of age (≤2.8%) as compared to younger participants (≤4.6%). (3) The frequency of serious adverse events was low (<0.5%), without meaningful imbalances between study arms. Among non-serious unsolicited adverse events, there were four cases of Bell’s palsy (facial paralysis) in the vaccine group (3, 9, 37, & 48 days post-vaccination) compared with no cases in the placebo group. Lymphadenopathy was imbalanced in the vaccine group (64) vs. the placebo group (6).
- COMMENTS: (1) The overall median duration of follow-up was less than 2 months. Therefore, no conclusions can be drawn on longer-term vaccine safety or efficacy at this stage. (2) Use during pregnancy and lactation, and in pediatric participants <16 years of age was not assessed. (3) The primary endpoint was evaluated in individuals without prior evidence of COVID-19 disease, thus excluding the possibility of assessing Antibody Dependent Enhancement (ADE) – see point 3 next). (5) Vaccine effectiveness against severe disease in at-risk demographics (i.e., hospital admissions, ICU admissions, mortality) and transmission of SARS-CoV-2 was not assessed. Remember, in a community setting it is the elderly with co-morbid disease who are at risk.
- EFFICACY COMMENT: Peter Doshi (Assoc. Editor BMJ): Pfizer and Moderna’s “95% effective” is cautioned. None of the leading vaccine candidate trials were designed to test if the vaccine can reduce severe COVID-19 symptoms (hospital admissions, ICU or death). Trials were also not designed to test if the vaccine can interrupt transmission (viral load, viral shedding, duration of viral shedding) https://www.bmj.com/content/bmj/371/bmj.m4037.full.pdf.
- POTENTIAL SARS-CoV-2 VACCINE SAFETY ISSUES: Antibody-dependent enhancement (ADE) of viral entry is a big concern and vaccine-associated enhanced disease (VAED).
- This EMA Petition by Dr. Michael Yeadon, former Chief Scientific Officer and VP for Pfizer Allergy Respiratory Research, details ADE as a potential safety issue: https://healthimpactnews.com/wp-content/uploads/sites/2/2020/12/Wodarg_Yeadon_EMA_Petition_Pfizer_Trial_FINAL_01DEC2020_EN_unsigned_with_Exhibits.pdf
- The scientific literature shows that if a human (macaque monkey, cat, or mouse) harbors a non-neutralizing antibody to a coronavirus through immunization (SARS-CoV, MERS, Feline Infectious Peritonitis, other), then a subsequent infection by the same virus can cause that person (or animal) to elicit a more severe immunological-inflammatory reaction to the virus and cause major disease or death (versus no immunization). This paradoxical immune response enhancement means vaccinated people and animals may be at a higher risk of developing disease or death than non-vaccinated people. “Normally” in vaccine development if there is immune enhancement in pre-clinical animal testing, this is a showstopper.
- Twenty-one citation links and abstract summaries are provided in the Excel file (Covid19 Vaccine Safety on page “Safety Issues”) linked to ADE. Click on the cells in the file to review the summary information or click the link and get the publications. This literature indicates that we must proceed with CAUTION with government mandated SARS-CoV-2 immunization. Alternatively, you can click on the hyperlinks at the bottom of this page to download the scientific publications.
- POTENTIAL SARS-CoV-2 VACCINE SAFETY ISSUES: Vaccine targeting of SARS-CoV-2 Spike (S) protein could cause infertility in women and men. This was not tested in clinical and pre-clinical studies (so far).
- DETERMINING VACCINE EFFICACY & DISEASE INCIDENCE (GENERALLY): the routine use of RT-PCR to diagnose SARS-CoV-2 infection results in high false-positives if the cycle thresholds (Ct) exceed 35 (i.e., in the USA, EU, UK a Ct of 40 is used).
- Read the EMA Petition sent by 3 experts, including Pfizer’s former CSO and VP of allergy and respiratory diseases. This is a highly critical review of Pfizer/BioNTech SARS-CoV-2 vaccine clinical study and its reliance on RT-PCR to confirm infection, without whole viral genome sequencing to confirm SARS-CoV-2 infection.
- Review-critique of the WHO promoted Corman Drosten protocol: Pieter Borger et al. “External peer review of the RT-PCR test to detect SARS-CoV-2 reveals 10 major scientific flaws at the molecular and methodological level: consequences for false positive results.” Cycle thresholds, unspecified oligonucleotide primer and probe sequences, and erroneous primer concentrations were major issues likely to facilitate high false-positive results. https://cormandrostenreview.com/report/.
- At a cycle threshold (Ct) of 25 up to 70% of patients remain viral positive in cell culture, and that at a Ct of 30 this value drops to 20%. At a Ct of 35 <3% of cultures are positive: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa1491/5912603.
- Tony Fauci CDC (16/07/2020): “…If you get [perform the test at] a cycle threshold of 35 or more…the chances of it being replication-competent [aka accurate] are miniscule… you almost never can culture virus [detect a true positive result] from a 37 threshold cycle…even 36…” (16/07/2020: at the 4.06 minute mark: https://www.youtube.com/watch?v=a_Vy6fgaBPE&feature=youtu.be&t=260)
- Publication: Correlation between successful isolation of virus in cell culture and Ct value of quantitative RT-PCR targeting E gene shows that patients with Ct above 33–34 are not contagious: https://link.springer.com/article/10.1007/s10096-020-03913-9.
Other issues of major concern:
- Was SARS-CoV-2 a genetically modified organism or bioweapon?
- Chimera virus: to exemplify that such research was conducted a zoonotic Chinese horseshoe bat RsSHC014-CoV spike protein was grafted onto a SARS-CoV mouse-adapted backbone in the USA. A 2015 publication shows how advanced this testing was, “A SARS-like cluster of circulating bat coronaviruses shows potential for human emergence” https://www.nature.com/articles/nm.3985. This collaborative program was funded under Gain-of-Function Research (i.e., bio-weaponization) Involving Influenza, MERS and SARS Viruses (http://www.phe.gov/s3/dualuse/Documents/gain-of-function.pdf). The study involved the University of North Carolina, the United States Army Medical Research Institute of Infectious Diseases, and the Wuhan Institute of Virology, among others.
- Chimera virus: Abstract excerpt: “to examine the emergence potential (that is, the potential to infect humans) of circulating bat CoVs, we built a chimeric virus encoding a novel, zoonotic CoV spike protein—from the RsSHC014-CoV sequence that was isolated from Chinese horseshoe bats—in the context of the SARS-CoV mouse-adapted backbone.”
- HIV inserts: Another publication was immediately retracted upon publication (https://www.biorxiv.org/content/10.1101/2020.01.30.927871v2): “Uncanny similarity of unique inserts in the 2019-nCoV spike protein to HIV-1 gp120 and Gag”. You can download an original PDF copy from this website or via: https://greatgameindia.com/uncanny-similarity-of-unique-inserts-in-the-2019-ncov-spike-protein-to-hiv-1-gp120-and-gag/
- HIV inserts: The 4 amino acid sequence insertions in the SARS-CoV-2 spike protein were not present in other coronaviruses analyzed (SARS, MERS, other). 3D modeling showed at least 3 of the HIV-like inserts converged to help form the receptor binding site (for viral entry). None of these HIV-like inserts are present in any other coronavirus, yet the rest of the SARS-CoV-2 spike protein is highly homologous with SARS and MERS viruses. This publication suggests this is “unlikely” to have occurred by chance.
- WHO reputation and strategic intent are called into question.
- WHO chief Tedros Adhanom Ghebreyesus said “widespread travel bans not needed to beat China virus” (02/07/2020), even though China had quarantined itself internally (https://www.reuters.com/article/us-china-health-who-idINKBN1ZX1H3). This failure to quarantine China led to the global spread of SARS-CoV-2.
- While WHO was telling the world not to quarantine China it was stalling to call a pandemic. This stalling was despite having already met WHO Stage 6 criteria for a pandemic (on ≥ 2 continents). A pandemic was finally called on 11/03/2020. This stalling to call the pandemic likely arose due to a WHO conflict of interest with the World Bank’s Pandemic Emergency Financing Facility (PEF Bonds). If WHO called a pandemic before the end of June 2020 then the Bond holders would forfeit c.$250mil of the $425mil bond. WHO was a non-executive of the PEF bond steering committee, as well as provider of the disease incidence data that would trigger bond clauses. https://www.worldbank.org/en/topic/pandemics/brief/pandemic-emergency-financing-facility, http://pubdocs.worldbank.org/en/882831509568634367/PEF-Final-Prospectus-PEF.pdf
- WHO stands accused of immunizing Kenyan women with an anti-fertility vaccine: Accordingly, WHO is said to have immunized young Kenyan women for “Tetanus” (Tetanus Toxoid) using a tetanus vaccine conjugated to human chorionic gonadotropin (hCG), without informed consent or disclosing the alterations to the vaccine. The vaccine was independently characterized and confirmed the presence of hCG: https://www.researchgate.net/publication/320641479_HCG_Found_in_WHO_Tetanus_Vaccine_in_Kenya_Raises_Concern_in_the_Developing_World, and https://pubmed.ncbi.nlm.nih.gov/12346214/ (WHO vehemently denied this allegation). Therefore, if this is TRUE then a WHO precedent already exists for covert-surreptitious fertility vaccination. Hence, the potential fertility issues linked to anti-Syncytin-1 antibodies must be taken seriously until confirmed otherwise.
- WHO (Tedros Adhanom Ghebreyesus) also stands accused of assisting genocide associated with the cholera epidemic in Sudan; https://www.genocidewatch.com/single-post/2017/07/24/an-open-letter-to-dr-tedros-adhanom-ghebreyesus-director-general-of-the-un-s-world-health).
- ISN’T IT STRANGE…? On the one hand WHO continues to hold the world vulnerable to an impending influenza pandemic by failing to recommend prepandemic immunization since the 2005 H5N1 zoonosis and 2009 swine flu pandemic. On the other hand it is pushing “hard” to ensure the world is immunized for a disease that this week (10/12/2020) had infected 0.88% of the world’s population (case fatality rates c.0.25% https://swprs.org/studies-on-covid-19-lethality/#overall-mortality). In 70 years, only WHO has made recommendations to change the flu vaccine definition; (1) annual seasonal flu vaccine redefinitions, and (2) adding a second Influenza-B antigen to the seasonal flu vaccine in 2013 (post-2009) so big Pharma could be induced to install more vaccine production capacity. Contrastingly, since 2009 key opinion leaders and vaccine company R&D leaders recommended pre-pandemic immunization. Big Pharma and WHO-Globalist politics won, while the world was left unnecessarily vulnerable to the next influenza pandemic. Pre-pandemic immunization would utilize vaccines composed of H5N1 and H7N9 (and other high risk threats) plus oil-in-water adjuvants to promote broadly cross-reactive antibodies. Such vaccines would enable much of the immunization process to be taken off the critical path allowing a population to be equitably immunized before the peak of a pandemic.
- When you hear Tedros Adhanom Ghebreyesus calling out on TV to national health authorities and the public to “TEST TEST TEST” that is arguably “code” to government healthcare service providers to ramp up their use of high false-positive RT-PCR diagnostic testing (Ct>35-40) to “fraudulently” hype-up the pandemic disease stats so they can fear monger the world (for their immunization agenda).
Antibody-Dependent Enhancement (ADE) publications
Antibody-Dependent Enhancement is a paradoxical immune response enhancement after vaccination (or natural infection) and means that vaccinated people (or animals) may be at a higher risk of developing disease or death than non-vaccinated people (or animals). “Normally” in vaccine development if there is immune enhancement in pre-clinical animal testing, this is a showstopper.
SARS-CoV-2
- Wen, J., Cheng, Y., Ling, R., Dai, Y., Huang, B., Huang, W., Zhang, S., & Jiang, Y. (2020). Antibody-dependent enhancement of coronavirus. International journal of infectious diseases: IJID : official publication of the International Society for Infectious Diseases, 100, 483–489. https://doi.org/10.1016/j.ijid.2020.09.015. (Publication link)
- Ulrich, H., Pillat, M.M. and Tárnok, A. (2020), Dengue Fever, COVID‐19 (SARS‐CoV‐2), and Antibody‐Dependent Enhancement (ADE): A Perspective. Cytometry, 97: 662-667. (Publication link)
- Arvin, A.M., Fink, K., Schmid, M.A. et al. A perspective on potential antibody-dependent enhancement of SARS-CoV-2. Nature 584, 353–363 (2020). https://doi.org/10.1038/s41586-020-2538-8. (Publication link)
- Salvatori, G., Luberto, L., Maffei, M. et al. SARS-CoV-2 SPIKE PROTEIN: an optimal immunological target for vaccines. J Transl Med 18, 222 (2020). https://doi.org/10.1186/s12967-020-02392-y. (Publication link)
- Cegolon L, Pichierri J, Mastrangelo G, et al. Hypothesis to explain the severe form of COVID-19 in Northern Italy. BMJ Global Health2020;5:e002564. doi:10.1136/bmjgh-2020-002564. (Publication link)
- Jason A. Tetro, Is COVID-19 receiving ADE from other coronaviruses?, Microbes and Infection, Volume 22, Issue 2, 2020, Pages 72-73, ISSN 1286-4579, https://doi.org/10.1016/j.micinf.2020.02.006. (Publication link)
- Kulkarni R. (2019). Antibody-Dependent Enhancement of Viral Infections. Dynamics of Immune Activation in Viral Diseases, 9–41. https://doi.org/10.1007/978-981-15-1045-8_2. (Publication link)
SARS-CoV & MERS
- Tseng C-T, Sbrana E, Iwata-Yoshikawa N, Newman PC, Garron T, et al. (2012) Immunization with SARS Coronavirus Vaccines Leads to Pulmonary Immunopathology on Challenge with the SARS Virus. PLoS ONE 7(4): e35421. doi:10.1371/journal.pone.0035421 (Publication link)
- Weingartl, H., Czub, M., Czub, S., Neufeld, J., Marszal, P., Gren, J., Smith, G., Jones, S., Proulx, R., Deschambault, Y., Grudeski, E., Andonov, A., He, R., Li, Y., Copps, J., Grolla, A., Dick, D., Berry, J., Ganske, S., Manning, L., … Cao, J. (2004). Immunization with modified vaccinia virus Ankara-based recombinant vaccine against severe acute respiratory syndrome is associated with enhanced hepatitis in ferrets. Journal of virology, 78(22), 12672–12676. https://doi.org/10.1128/JVI.78.22.12672-12676.2004 (Publication link)
- Luo, F., Liao, F. L., Wang, H., Tang, H. B., Yang, Z. Q., & Hou, W. (2018). Evaluation of Antibody-Dependent Enhancement of SARS-CoV Infection in Rhesus Macaques Immunized with an Inactivated SARS-CoV Vaccine. Virologica Sinica, 33(2), 201–204. https://doi.org/10.1007/s12250-018-0009-2. (Publication link)
- Yip MS, Leung NH, Cheung CY, Li PH, Lee HH, Daëron M, Peiris JS, Bruzzone R, Jaume M. Antibody-dependent infection of human macrophages by severe acute respiratory syndrome coronavirus. Virol J. 2014 May 6;11:82. doi: 10.1186/1743-422X-11-82. PMID: 24885320; PMCID: PMC4018502. (Publication link)
- Wang, S. F., Tseng, S. P., Yen, C. H., Yang, J. Y., Tsao, C. H., Shen, C. W., Chen, K. H., Liu, F. T., Liu, W. T., Chen, Y. M., & Huang, J. C. (2014). Antibody-dependent SARS coronavirus infection is mediated by antibodies against spike proteins. Biochemical and biophysical research communications, 451(2), 208–214. https://doi.org/10.1016/j.bbrc.2014.07.090. (Publication link)
- Zhi-yong Yang, Heidi C. Werner, Wing-pui Kong, Kwanyee Leung, Elisabetta Traggiai, Antonio Lanzavecchia, Gary J. Nabel, Evasion of antibody neutralization in emerging severe acute respiratory syndrome coronaviruse. Proceedings of the National Academy of Sciences Jan 2005, 102 (3) 797-801; DOI: 10.1073/pnas.0409065102. (Publication link)
- Yushun Wan, Jian Shang, Shihui Sun, Wanbo Tai, Jing Chen, Qibin Geng, Lei He, Yuehong Chen, Jianming Wu, Zhengli Shi, Yusen Zhou, Lanying Du, Fang Li, Molecular Mechanism for Antibody-Dependent Enhancement of Coronavirus Entry. Journal of Virology Feb 2020, 94 (5) e02015-19; DOI: 10.1128/JVI.02015-19. (Publication link)
Feline Infectious Peritonitis (FIP) vaccination enhances FIP disease upon infection
- Pathogenesis of oral type I feline infectious peritonitis virus (FIPV) infection: Antibody-dependent enhancement infection of cats with type I FIPV via the oral route. (Publication link)
- Hohdatsu, T., Nakamura, M., Ishizuka, Y., Yamada, H., & Koyama, H. (1991). A study on the mechanism of antibody-dependent enhancement of feline infectious peritonitis virus infection in feline macrophages by monoclonal antibodies. Archives of virology, 120(3-4), 207–217. https://doi.org/10.1007/BF01310476. (Publication link)
- Vennema, H., de Groot, R. J., Harbour, D. A., Dalderup, M., Gruffydd-Jones, T., Horzinek, M. C., & Spaan, W. J. (1990). Early death after feline infectious peritonitis virus challenge due to recombinant vaccinia virus immunization. Journal of virology, 64(3), 1407–1409. https://doi.org/10.1128/JVI.64.3.1407-1409.1990. (Publication link)
- Weiss, R. C., & Scott, F. W. (1981). Antibody-mediated enhancement of disease in feline infectious peritonitis: comparisons with dengue hemorrhagic fever. Comparative immunology, microbiology and infectious diseases, 4(2), 175–189. https://doi.org/10.1016/0147-9571(81)90003-5. (Publication link)
- Tomomi TAKANO, Chisako KAWAKAMI, Shinji YAMADA, Ryoichi SATOH, Tsutomu HOHDATSU, Antibody-Dependent Enhancement Occurs Upon Re-Infection with the Identical Serotype Virus in Feline Infectious Peritonitis Virus Infection, Journal of Veterinary Medical Science, 2008, Volume 70, Issue 12, Pages 1315-1321, Released January 01, 2009, Online ISSN 1347-7439, Print ISSN 0916-7250, https://doi.org/10.1292/jvms.70.1315, https://www.jstage.jst.go.jp/article/jvms/70/12/70_12_1315/_article/-char/en. (Publication link)
- Hohdatsu T, Yamada M, Tominaga R, Makino K, Kida K, Koyama H. Antibody-dependent enhancement of feline infectious peritonitis virus infection in feline alveolar macrophages and human monocyte cell line U937 by serum of cats experimentally or naturally infected with feline coronavirus. J Vet Med Sci. 1998 Jan;60(1):49-55. doi: 10.1292/jvms.60.49. PMID: 9492360. (Publication link)
- Takano, T., Nakaguchi, M., Doki, T., & Hohdatsu, T. (2017). Antibody-dependent enhancement of serotype II feline enteric coronavirus infection in primary feline monocytes. Archives of virology, 162(11), 3339–3345. https://doi.org/10.1007/s00705-017-3489-8. (Publication link)
by Carlton Brown | Sep 22, 2020 |
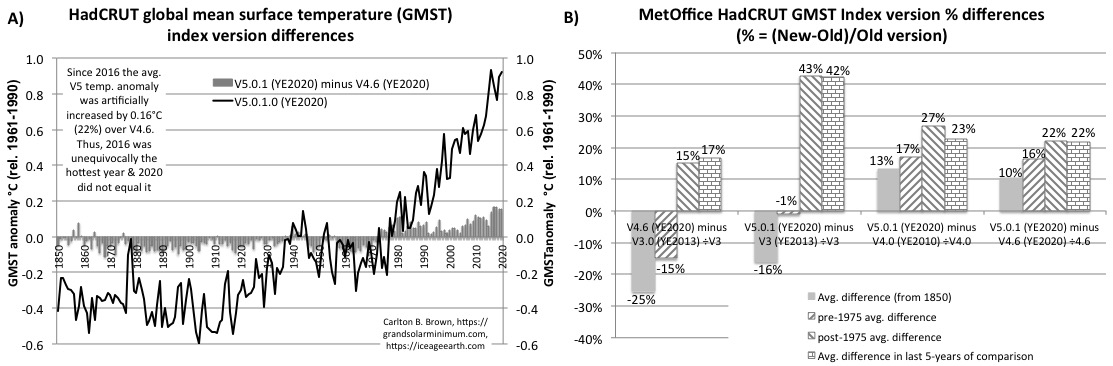
It is impossible to know what happened to the global surface temperature between 1850/1880 and 2020 utilizing the global surface temperature indices provided by NASA, National Oceanic and Atmospheric Administrations (NOAA), and the MetOffice, without access to the raw data. This situation arises because all current temperature indices have been majorly altered over earlier versions, which is evidenced by subtracting the old from the new versions. These index version changes had the effect of increasing the warming rate and absolute temperature increase from 1900 to 2020 while giving the impression that 2020 was broadly on par with or exceeded an artificially diminished 2016 peak temperature.
Data Sources: see the data hyperlinks in the table below. This data was provided and altered by NASA, National Oceanic and Atmospheric Administration (NOAA), and the UK MetOffice.
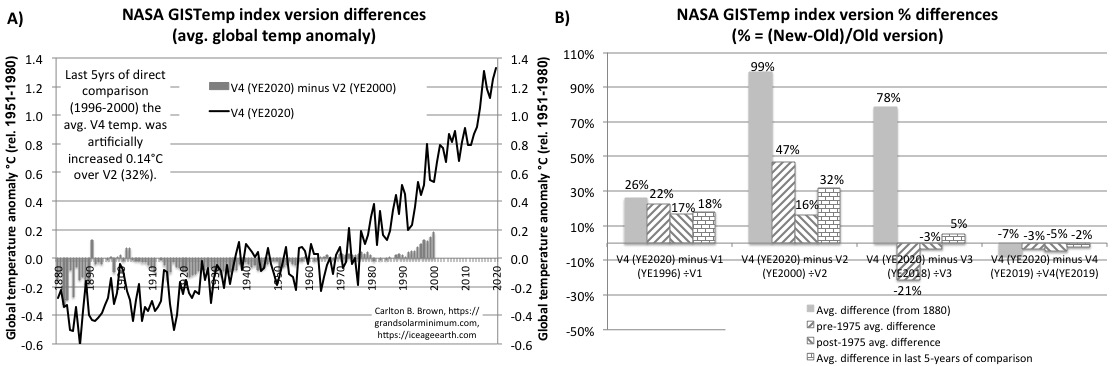
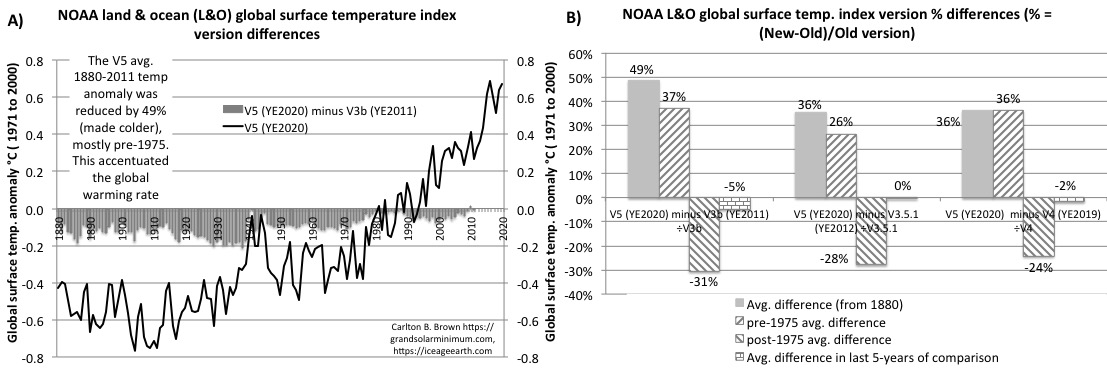
Figure legend: Version differences for MetOffice NASA, and NOAA global mean surface temperature indices (current versus predecessors). Subtracting the older index version from the current version revealed the differences. Annual global temperature anomaly differences were averaged by period groupings into start-to-end, pre-1975 and post-1975, and the last 5-years. The period grouping percentage differences were calculated (%={new version minus old version} /divided by old version). A positive percentage before 1975 meant an increased cooling, while a positive percentage after 1975 meant increased warming. A negative percentage before 1975 meant a reduced cooling, while a negative percentage after 1975 meant reduced warming.
When HadCRUT current V5.0.1 (YE2020) version was compared with its predecessor V4.6 (YE2020), V4.0 (YE2010), and V3 (YE2013) versions; the post-1975 average temperature anomaly (rel. 1961-1990) was increased by 22%-43%, and the last 5-years of direct comparison were increased by 22%-42% (made warmer) over the earlier versions. The pre-1975 average temperature anomaly was reduced by 16-17% (made colder) for V5.0.1 over the V4.6 and V4.0 versions. The largest warming increases were observed between V5.0.1 over V3 for the post-1975 period (43%) and the last 5-years of comparison (42%, 2009-2013). These post-1975 changes had the effect of making 2020 broadly on par with the prior 2016 peak global temperature.
NASA’s current V4 version (YE2020) average temperature anomaly (1880-to-end, rel.1951-1980) increased by 99% over V2 (YE2000, made colder), 78% over V3 (YE2018, made warmer), and by 26% over V1 (YE1996, made colder). The largest version differences were observed between V4 (YE2020) over V2 (YE2000) across all comparator periods (16%-99%). The average 1880-to-end difference increased by 99% (made colder), the pre-1975 was reduced by 47% (made colder), while the last 5-years of direct comparison saw the V4 warming increase by 32% (1996-2000). NASA’s V4 (YE2020) adjustments over its V4 (YE2019) version also reduced the 2016 peak temperature anomaly from 1.33°C to 1.31°C, reduced the 2019 temperature anomaly from 1.28°C to 1.25°C, thus making 2020 the hottest year (1.33°C), which usurped an artificially diminished 2016 peak temperature in the hottest temperature rankings.
NOAA’s current V5 version (YE2020) average anomaly (1880-to-end, rel.1971-2000) increased by 36-49% over the V4 (YE2019), V3.5.1 (YE2012), and V3b (YE2011) versions (made colder in all cases) with most of the change occurring pre-1975 (26-37%). NOAA’s V5 (YE2020) adjustments also increased the temperature anomaly in 2019 by 0.03°C (5%) over V4 (YE2019), while reducing the 2016 peak temperature 0.02°C. These changes made 2020 broadly on par with a diminished 2016 global peak temperature in the hottest temperature rankings.
by Carlton Brown | Mar 14, 2020 |
The first scientific paper to expose the potential genetic engineering of the coronavirus (COVID19). This paper was WITHDRAWN after being posted at Cold Spring Harbor Laboratory (Click this link). “Uncanny similarity of unique inserts in the 2019-nCoV spike protein to HIV-1 gp120 and Gag,” Click this link to a downloadable PDF 2020.01.30.927871.full
by Carlton Brown | Nov 25, 2019 |
MS Word version (navigable links): Scientific Refutation_IPCC Key Risk Assessment AR5_House of Lords
PDF Slide deck summary: Scientific Refutation of IPCC AR5 Key Risk Assessment_UK
Email recipients: See the House of Lords (UK) email recipients below.
Subject: XXX
by Carlton Brown | Nov 12, 2019 |
MS Word version (navigable citation links): Scientific-Refutation-of-the-IPCCs-Key-Risk-Assessment_NZ_Final
PDF Slide deck summary: Scientific Refutation of the IPCC-AR5 Key Risk Assessment
Email recipients: See all To and Copied recipients below (not the BCC-ed).
Subject: Request for Investigation: the UN/IPCC’s corruption of climate science results in Prime Minister Jacinda Ardern lying to the public
Dear Prime Minister, Ministers and Associate Ministers of Education, Justice and Broadcasting/Communications/Media, the Attorney General, and Universities New Zealand Vice-Chancellors
Would you please investigate the corruption of normal-science in the climate science field (“corruption”) by the Intergovernmental Panel on Climate Change (“IPCC”), and its impact on New Zealand academia and student miseducation, on government policies and media, and on future human safety? With Prime Minister Jacinda Ardern blatantly lying in contradiction to the 2019 climate data (“lie”), “We’re here because our world is warming. Undeniably it is warming,” it is clear this corruption has undermined government objectivity. Between early 2016 and mid-2019 global temperatures declined 0.47°C, telling us the world is “undeniably cooling.”
The only climate change key-risk assessment that matters to this government is what the IPCC contrived under a United Nations Framework Convention on Climate Change (UNFCCC) Article-2 diktat in its Fifth Assessment Report (AR5, see Minister Shaw’s letter) linked only to theoretical anthropogenic global warming (AGW). This UN-diktat resulted in the erroneous dismissal of catastrophic natural climate change risks most relevant to the 21st century, just to eliminate any cooling contestation to the IPCC’s policy-directing Representative Concentration Pathway global warming scenarios. The Ministry for the Environment’s National Climate Change Risk Assessment (NCCRA, NCCRAF master templates) was also constrained by this UNFCCC Article-2 dictated risk-framework and predetermined the theoretical anthropogenic global warming risks upfront, before dressing it up with a Maori name (“Arotakenga Huringa Āhuarangi”) and then giving it to the assessment team.
The expert credentials of anyone promoting the IPCC’s Article 1 and 2 dictated sham-science and key-risk assessment are called into question if they failed to critically review all 4,931 pages of AR5 against the unfiltered climate data and science detailing our catastrophic natural climate change history back to the Holocene Climate Optimum, and thus failed to;
- Realize the major fabrication of global warming by UK and US government agencies (MetOffice, NOAA, NASA), evidenced by subtracting the post-1990 global climate index versions from the current versions. These fabricated global climate indices are those used by the IPCC and New Zealand’s government (MFE) to manipulate public opinion and justify policy.
- Realize that global atmospheric temperatures declined 0.47°C between early 2016 and mid-2019, while carbon dioxide (CO2) increased 2.8%. In AR5 the IPCC projected a 2016-2035 global mean surface temperature (GMST) increase of 0.3°C-0.7°C, meaning its policy-directing forecast is in error.
- Refute the IPCC’s radiative forcing theory based on its three-decade legacy for generating highly inaccurate climate forecasts (AR5): 1986-1998; 84% under-forecasted the GMST. 1998-2012; 97% over-forecasted GMST, while 100% failed to predict the 15-year climate hiatus (no GMST increase) during this same period when CO2 increased by 8.0%. Points 2 and 3 clearly show the IPCC theory is unable to predict the GMST and its natural oscillations.
- Realize the modern era’s natural warming phase actually started in the depths of the Little Ice Age (early 1700s) and long before significant human greenhouse gas emissions. This fact of data is veiled from public view by the IPCC’s reliance on fabricated global climate indices that started between 1850 and 1880CE i.e., UNFCCC Article 1 defined climate change and AGW hijacked/rebranded natural climate change.
- Reflect that a major glaciation started after the Holocene Climate Optimum, which tracked a 40-50Watt/m2 decline in solar irradiance over eight millennia (i.e., 15 times today’s putative human radiative forcing impact) and a near 5°C decline in Arctic/Antarctic ice core temperatures by 1700CE (20%/36% of their Holocene interglacial rise, in absolute terms). This glaciation peaked during the Little Ice Age, and its melt initiation preceded significant human activity. Despite five-millennia of glaciation up to the mid-19th century, the IPCC erroneously dismissed with virtual certainty the prospect of glaciation for the next 1,000 years.
- Refute the IPCC’s non-peer reviewed mini-theory that delayed the next ice age by an unprecedented 30,000-50,000 years, and to falsify its incorrect assumption that the last ice age ended ‘about 10,000 years ago.’ Minister James Shaw as minister of statistics ignored a major statistical oversight that would normally falsify this ice age delay theory on three counts, never mind its conflict with existing climate data.
- Critically question the IPCC’s key-risk assumption that climate change risk lessons from the Little Ice Age and rapid climate change events since just before the Holocene Climate Optimum, associated with famine, war, and epidemic related catastrophes, civilization destructions, and species extinctions, were not applicable today.
- Realize that the IPCC erroneously dismissed or omitted catastrophic natural climate change risks most relevant to the 21st century, and which have been in plentiful evidence over the last eight millennia, i.e., global cooling cycles, glaciation, climate-forcing volcanism, grand solar minimum related extremes of precipitation (±), rapid climate change, and pandemic influenza.
- Reflect the alternative 21st-century climate forecasts from leading solar activity scientists expert in climate change, who warn of a return to a Little Ice Age-like climate during this current grand solar minimum period. Is this why cold, snow and precipitation records are being shattered all around the world in 2019?
- Realize that a detailed correlation analysis between CO2 and the GMST does not support their cause and effect relationship. This explains the IPCC’s high forecast inaccuracy and why a correlation analysis was not provided in any IPCC Working Group 1 report since 1990.
- Realize governments and corporates only have fifty years of ‘proven’ oil and gas reserves on their balance sheets, which is insufficient to generate the full 21st-century global warming that we are fear-mongered with, let alone delay an ice age. With reserves-to-production for oil and gas being less than 100% for most of the last 40 years, peak discovery is history. As such, all IPCC climate forecasts are technically invalidated.
On the basis of points 1-11 the IPCC’s radiative forcing (RF) theory, forecasts, and key-risk assessment would normally be refuted and replaced had the climate science field not been corrupted by UNFCCC Articles 1 and 2, IPCC processes and procedures, government-directed academic funding, and other factors.
In the event of an unmitigated 21st-century natural climate change catastrophe, blindly-following UN member state governments, the international scientific community, and the world’s media could be considered complicit in a UN/IPCC-led strategic genocide (“genocide”), consequent to this corruption. By implementing dubious UN global strategies into national policy and strategies this government places our nation and economy at risk (i.e., (1) IPCC/NCCRA; unmitigated catastrophic natural climate change risks. (2) WHO/MOH; enforcing our vulnerability to pandemic influenza during this high-risk grand solar minimum period by following an obsolete global vaccine strategy), while undermining our nation’s self-determinism and sovereignty.
Because the 1988 UNFCCC Article 1 and 2 dictated sham-science paradigm dominates New Zealand academia and tertiary miseducation the request to investigate this corruption is relevant to the minister of education and to the university vice chancellors. The high-possibility for 21st-century genocide resulting from United Nations global strategies benefiting from this corruption and being implemented by this government make this request a legal and human rights issue relevant to the minister of justice and the attorney general. The fact New Zealand’s media have failed to investigate this corruption, which sees our Prime Minister and minister of climate change publicly lie in contradiction to the climate data, makes this request relevant to the minister of broadcasting, communications and digital media – and the Prime Minister herself.
The following attached documents will show you exactly where to look in AR5’s 4,931 pages to see the IPCC’s incriminating disclosures and will help you understand the natural climate change risks, data, and science that was filtered out by the IPCC’s corruptive process.
- Scientific Refutation (MS Word): https://grandsolarminimum.com/wp-content/uploads/2019/11/Scientific-Refutation-of-the-IPCCs-Key-Risk-Assessment_NZ_Final.docx
- Slide deck (PDF): https://grandsolarminimum.com/wp-content/uploads/2019/11/Scientific-Refutation-of-the-IPCC-AR5-Key-Risk-Assessment.pdf
See my credentials below my signature.
Thank you.
Dr. Carlton Brown BVSc (Massey University) MBA (London Business School)
Advocate for Natural Climate Change Risk-Mitigation: Switching to Renewable Energy, and Implementing Centralized/Decentralized Sustainable Development and Prepandemic Influenza Immunization (Urgently)
FreeBook “Revolution: Ice age Re-entry”: Regular Amazon #1 (https://amzn.to/2PyQsxV), Google Play (http://bit.ly/2JFHz08), Kobo (http://bit.ly/2F3DdRQ), and Researchgate (http://bit.ly/2UnTBju)
LinkedIn: https://www.linkedin.com/in/carlton-brown-13b66232/
Website: https://grandsolarminimum.com
Twitter: https://twitter.com/Iceagereentry
Copyright © 2014 Carlton B. Brown of https://grandsolarminimum.com. All Rights are Reserved. You are free to forward this information on to third parties and use this information under CC-BY-SA 4.0 rules.
My research credentials and link to pandemic influenza, climate change, and earth system risks: See my LinkedIn profile.
I am a New Zealand graduated veterinarian (Massey University, 1987), with an MBA (London Business School, 1997) and commercial background in human life sciences (UK; Pharma, Biotech, Investment Banking). As co-founding CEO/co-lead scientist of Immune Targeting Systems Ltd, I spent a decade directing the innovation and development of a universal pandemic influenza vaccine able to immunologically target all potential pandemic influenza-A strains in a genetically diverse human population. The company also assessed the broadly cross-reactive antibody responses (able to target emerging viral mutants) of all regulatory approved vaccine adjuvants in combination with influenza hemagglutinin antigens (i.e., seasonal and pandemic influenza vaccine antigens). As CEO I raised NZ$47million from European life-science investors and directed the vaccine technology innovation and development from inception to human proof-of-concept clinical studies, including breaking a global monopoly on the conduct of human influenza challenge studies. The company was sold in 2015.
That vaccine innovation project catalyzed my interest in influenza viral mutation epidemiology, and the role of Arctic migrating birds carrying pre-pandemic influenza-A viruses into cyclical extremes of electromagnetism, geomagnetism, and natural climate change during their summer migration. This resulted in the discovery that pandemic influenza outbreaks since 1500CE (the Little Ice Age) biased 11-year solar minimum/maximum periods, and grand solar minimum periods linked to Arctic cooling and glaciation. This discovery was facilitated by analyzing more than 100 data sets and many permutations of correlations between solar electromagnetism and magnetism, geomagnetism, climate change, glaciation, volcanism, and influenza pandemics, which made the lie about anthropogenic global warming and the error of our glacial cycle stage blatantly obvious.
Email recipients:
To: c.hipkins@ministers.govt.nz, j.salesa@ministers.govt.nz, k.davis@ministers.govt.nz, t.martin@ministers.govt.nz, david.parker@parliament.govt.nz, a.little@ministers.govt.nz, jan.logie@parliament.govt.nz, a.sio@ministers.govt.nz, kris.faafoi@parliament.govt.nz, s.mccutcheon@auckland.ac.nz, neilq@waikato.ac.nz, J.B.Thomas@massey.ac.nz, hayne@psy.otago.ac.nz, vice-chancellor@otago.ac.nz, vice-chancellor@vuw.ac.nz, cheryl.delarey@canterbury.ac.nz, Bruce.McKenzie@lincoln.ac.nz, VCOffice@lincoln.ac.nz, derek.mccormack@aut.ac.nz, jacinda.ardern@parliament.govt.nz,
CC-ed: winston.peters@parliament.govt.nz, james.shaw@parliament.govt.nz, eugenie.sage@parliament.govt.nz, nanaia.mahuta@parliament.govt.nz, Megan.Woods@parliament.govt.nz, Damien.O’Connor@parliament.govt.nz, phil.twyford@parliament.govt.nz, shane.jones@parliament.govt.nz, julieanne.genter@parliament.govt.nz, willow-jean.prime@parliament.govt.nz, david.clark@parliament.govt.nz, peeni.henare@parliament.govt.nz, ron.mark@parliament.govt.nz, Stuart.nash@parliament.govt.nz
Recent Comments